Most Popular
-
1
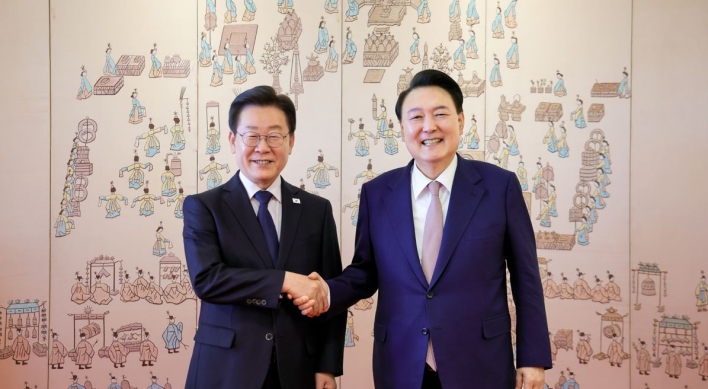
Tensions heighten ahead of first president-opposition chief meeting

-
2
Seoul to provide housing subsidy to married couples with newborns

-
3
[KH Explains] No more 'Michael' at Kakao Games
![[KH Explains] No more 'Michael' at Kakao Games](//res.heraldm.com/phpwas/restmb_idxmake.php?idx=644&simg=/content/image/2024/04/28/20240428050183_0.jpg&u=20240428180321)
-
4
Rapper jailed after public street fight with another rapper

-
5
Woman gets suspended term for injuring boyfriend with knife



![[KH Explains] No more 'Michael' at Kakao Games](http://res.heraldm.com/phpwas/restmb_idxmake.php?idx=644&simg=/content/image/2024/04/28/20240428050183_0.jpg&u=20240428180321)


-
6
Samsung chief bolsters ties with Germany’s Zeiss

-
7
NewJeans pops out ‘Bubble Gum’ video amid troubles at agency

-
8
Med schools expect 1,500+ new admission slots next year

-
9
[Grace Kao] Hybe vs. Ador: Inspiration, imitation and plagiarism
![[Grace Kao] Hybe vs. Ador: Inspiration, imitation and plagiarism](//res.heraldm.com/phpwas/restmb_idxmake.php?idx=644&simg=/content/image/2024/04/28/20240428050220_0.jpg&u=)
-
10
Nominee for chief of anti-corruption body pledges 'independence, effectiveness'




![[Grace Kao] Hybe vs. Ador: Inspiration, imitation and plagiarism](http://res.heraldm.com/phpwas/restmb_idxmake.php?idx=644&simg=/content/image/2024/04/28/20240428050220_0.jpg&u=)

[Contribution] 6 reasons why medical school expansion isn’t the answer
By Korea HeraldPublished : April 16, 2024 - 12:54

I’m Ryu Ok Hada, a trainee doctor who resigned from the Catholic Medical Center on Feb. 16.
Recently, President Yoon Suk Yeol said that the medical community should come up with a unified proposal on an appropriate increase in the annual medical school admissions quota based on scientific and rational grounds.
A survey I conducted on 1,581 trainee doctors and medical students between March 29 and April 1 showed that 96 percent of the respondents think that the increase in the medical school enrollment quota should be either reduced or that the quota should be held as it is. I would like to explain why 96 percent of young doctors are against it.
Firstly, the number of doctors in South Korea has steadily increased, even without the medical school quota hike. While the medical school quota has been frozen at 3,058 for 27 years, the admissions quota was between 800 and 1,040 when now-retired doctors entered medical schools.
Compared to the number of doctors who have retired, the number of new doctors has increased nearly 2.9 to 3.8-fold, resulting in rapid growth in the total number of active physicians from approximately 87,000 in 2012 to 112,300 in 2020. This means that, while the quota has been frozen, the number of doctors hasn’t.
Secondly, the plan to increase the number of medical students will affect patient health and their experience. Under the current “fee-for-service” system, a payment model in which doctors are paid based on the number of medical services they provide, physicians have an incentive to perform more medical procedures.
However, having more doctors will create supplier-induced demand, and patients may find themselves in situations where they receive expensive treatment and shorter appointments. Hence, an increase in medical school places will not only increase health insurance premiums and reduce coverage but will also accelerate health care commercialization.
Thirdly, an estimate of the number of doctors needed should consider several additional factors. One of the reports the government relied on to justify the expansion of medical schools, written by professor Hong Yun-Chul of Seoul National University, gauged that the country would fall short of 7,264 doctors in 2035. But the report also noted that strengthening primary health care would reduce that figure to 2,637, suggesting that health care reform is more important.
Furthermore, considering the factors overlooked by the three reports that the government used to decide on the expansion plan, there is certainly room for reducing the medical school enrollment quota. One factor to consider is the “healthy aging effect,” which takes the healthy lifespan of older people into account. A delay in doctors’ retirement age should also be considered.
Fourth, advancements in medical technology are expected to reduce the demand for health care overall. Before, patients would undergo surgeries to remove a part of the stomach for minor stomach cancer and spend about a week in the hospital. Now, for early-stage stomach cancer, patients can go through endoscopic treatment and stay at the hospital for about three days. The rapid progress in artificial intelligence and synthetic biology will undoubtedly accelerate such changes.
Fifth, increasing the medical school quota will only deteriorate the quality of education. Even if we increase the quota, an increase of 2,000 places is not realistic.
In a medical education approach involving a systematic and specialized structure that ranges from basic science to clinical medicine, clinical practice and residency, a sudden increase in the quota will only lead to increasing the number of medical licenses rather than nurturing high-quality doctors. Adequate time is needed to find professors for basic medicine, classrooms, cadavers for anatomy classes and to create practical hospital environments.
Sixth, increasing medical school admissions is not a solution that could salvage regional health care. Providing one-time cash support or forcing doctors to work at such places alone cannot attract doctors to rural areas. Simply placing doctors in rural areas when kindergartens, convenience stores and schools are closing due to regional decline will not solve the problem of medical vulnerability in those areas.
Similarly, merely increasing the number of medical schools in rural areas will inevitably result in differences in the quality of education and training compared to medical schools in the capital region. Patients will not trust doctors and hospitals developed in such environments, and medical tourism to Seoul will speed up, exacerbating the local extinction crisis.
Health care reform is necessary, but increasing medical school enrollment is not the answer.
I would like to propose a demand-driven approach to health care reform that can be implemented immediately, rather than a medical school expansion that will take 10 to 20 years and may not even be effective.
This alternative focuses on curbing excessive medical usage and restoring the health care delivery system. We should revive regional health care by protecting doctors who practice medicine in good faith from legal risks, ensuring high-quality specialist education in specialist-centric hospitals and restructuring health care around patient-centered care.
In this case, discussions about medical school expansion may become unnecessary in the future.
By Ryu Ok Hada
Ryu Ok Hada is a trainee doctor who resigned from the Catholic Medical Center. The views expressed in this article are his own. -- Ed.
-
Articles by Korea Herald